Meeting Date: January 11, 2019
Report No.: BH.01.JAN1119.R02
Prepared By: Courtney Bell, Health Promotion Specialist, Healthy Communities and Public Policy; Amy Estill, Manager, Healthy Communities and Public Policy
Approved By: Dr. Matthew Tenenbaum, Acting Director, Family Health
Submitted By & Signature: Dr. Nicola J. Mercer, MD, MBA, MPH, FRCPC Medical Officer of Health & CEO
Recommendations
It is recommended that the Board of Health:
- Receive this report for information.
Key Points
- An anonymous and voluntary online survey was administered to Wellington-Dufferin-Guelph (WDG) residents between June 7, 2018 and July 8, 2018. It included questions about attitudes toward cannabis use, knowledge of the health effects of cannabis, interest in using cannabis once legal, current cannabis use behaviours, and impacts of cannabis use.
- Over one-third of respondents indicated that they had used cannabis in the past year. This finding is higher than recent Canada-wide surveys that suggest that approximately 15 to 22 percent of the population has used cannabis in the past year.
- Among respondents who reported that they have not used cannabis in the past year, over half of them reported they are not likely to try cannabis once it is legal in Canada.
- Most respondents believed that cannabis use was beneficial, socially acceptable, and it would be easy for them to access cannabis in the next 24 hours.
- The survey identified various knowledge gaps around cannabis use and its related harms. People who had used cannabis in the past year were less likely to know about the health effects of cannabis compared to people who had not used cannabis in the past year.
Discussion
Background
In June 2018, the Federal government passed Bill C-45, the Cannabis Act, which legalizes, regulates and controls the production, distribution and sale of cannabis and allows adults to legally possess cannabis. The goals of the Cannabis Act include: keeping cannabis out of the hands of youth, keeping the profits out of the hands of criminals, and protecting public health and safety by allowing adults access to safe and legal cannabis.1 Cannabis became legal in Canada on October 17, 2018.
Currently in Ontario, the only legal option for purchasing non-medical cannabis is online through the Ontario Cannabis Store (OCS). By April 1, 2019, the province is expecting to launch a retail model for cannabis that will be regulated by the Alcohol and Gaming Commission of Ontario.2 The Federal government plans to authorize the sale of cannabis edible products at the federal, provincial and territorial levels within twelve months of the Cannabis Act being released. 2
These legal changes will likely have impacts on cannabis use patterns in Canada. Public health evidence from alcohol and tobacco shows that increased access to a substance tends to result in greater consumption and harms.3,4 To assess and monitor the impact that legalization has in Canada, it is important to collect information on the frequency of cannabis use and changes in behaviour over time. Other surveys, including the Canadian Tobacco, Alcohol, and Drugs Survey (CTADS); the National Cannabis Survey (NCS); and the Canadian Cannabis Online Survey (CCOS) collect information on cannabis use among Canadians, however the results are not available at the local level.5,6,7
To fill this information gap, Wellington-Dufferin-Guelph Public Health (WDGPH) administered a survey in June of 2018 to gather baseline information about people’s attitudes towards cannabis, their knowledge of its health effects, their interest in using cannabis once legal, their cannabis use behaviours, and the impacts of cannabis use on current users. This information will serve as a baseline to compare with surveys conducted in the future, to assess the impacts of the legalization on cannabis use patterns. Additionally, the information can be used by WDGPH and community partners to guide the development of educational resources and interventions to address the potential impacts of cannabis legalization.
Methods
An anonymous and voluntary online survey was administered to WDG residents ages 16 and older between June 7, 2018 and July 8, 2018. Respondents were recruited using online and print advertising, and the survey was promoted through local media. Targeted advertisements were used to increase the response rate among underrepresented communities.
After the survey results were collected, responses were weighted using local census data for age, education and gender to make the sample more representative of the WDG population. Responses from people who have used cannabis in the past 12 months (cannabis “users”) were compared with responses from people who have not used cannabis in the past 12 months (cannabis “non-users”). Results were analyzed to determine if differences between these groups were statistically significant.
Results
Individuals could choose whether or not to participate in the WDG Cannabis Survey, so respondents were not a random sample. Results should be interpreted with caution, since individuals who chose to participate may be different than individuals who chose not to participate.
Respondent Demographics
A total of 4,073 survey responses were received, of which 2,776 were valid and complete. The sample included a high proportion of females, people who have completed a post-secondary education and people 20 to 39 years of age. Table 1 shows the demographics of respondents before and after weighting to match local census data.
| Demographic category | Variable | Original survey sample | Census-weighted sample |
|---|---|---|---|
| Cannabis use | Past year cannabis use | 40.1% | 38.3% |
| Gender | Male | 28.7% | 46.7% |
| Female | 70.3% | 53.3% | |
| Age | 19 and under | 5.4% | 7.6% |
| 20-29 | 24.1% | 16.6% | |
| 30-39 | 25.8% | 16.6% | |
| 40-49 | 19.3% | 16.3% | |
| 50-59 | 15.2% | 20.2% | |
| 60-69 | 7.8% | 15.2% | |
| 70+ | 2.3% | 7.6% | |
| Highest level of education | Elementary school | 2.8% | 11.4% |
| High school diploma | 22.5% | 30.9% | |
| Trade certificate | 3.8% | 7.6% | |
| College diploma/certificate | 29% | 22.9% | |
| University degree | 41.9% | 27.2% |
Cannabis Knowledge
Participants were asked how much they agree with a series of knowledge-based questions about the health risks associated with using cannabis. Table 2 shows the percent that agree among all respondents, among people who use cannabis and among people who do not use cannabis.
| Agree (%) | |||
|---|---|---|---|
| Knowledge statement | All respondents | People who use cannabis | People who do not use cannabis |
|
Using cannabis before driving increases your risk of a motor vehicle collision [TRUE] |
82.5% | 74.3% | 84.3% |
|
Using cannabis while pregnant can cause harm to the fetus/child [TRUE] |
66.4% | 58.2% | 69.2% |
|
Using cannabis daily or almost daily can cause problems with memory, learning and decision-making [TRUE] |
56.6% | 44.4% | 60% |
|
Using high doses of cannabis can cause psychosis (losing touch with reality) [TRUE] |
51.3% | 35.7% | 52.5% |
|
Using cannabis may result in dependence or addiction [TRUE] |
47.6% | 32.7% | 48.2% |
|
Cannabis smoke has many of the same cancer-causing chemicals as tobacco smoke [TRUE] |
38.2% | 25.9% | 42.3% |
|
Youth (under 25 years old) and adults have the same level or risk for harms related to cannabis [FALSE] |
25.1% | 19% | 26.8% |
Note: Table includes people who ‘strongly agree’ and ‘somewhat agree’.
Note: All differences between people who use cannabis and people who do not are statistically significant.
The majority of respondents were not able to identify the correct response. For most statements, fewer than two-thirds of respondents agreed with the correct response. For example, only 38.2% of respondents agreed that cannabis smoke has the same cancer-causing chemicals as tobacco smoke These results highlight the importance of WDGPH and partners improving knowledge about cannabis use.
People who had used cannabis in the past year were less likely to identify the correct response than people who had not used cannabis in the past year. This was most evident for the statements about cognitive and mental health impacts of cannabis use. It is particularly important that cannabis users have accurate information to inform their behavior.
Respondents were also asked if they had heard of Canada’s Lower-Risk Cannabis Use Guidelines, developed by the Centre for Addictions and Mental Health (CAMH). The guidelines include ten (10) evidence-informed recommendations which suggest ways to use cannabis more safely. Most respondents (87.2%) indicated that they had not heard of these guidelines.
Attitudes towards Cannabis
Participants were asked how much they agreed with a series of attitude-based questions about cannabis. Table 3 shows the percent that agree among people who use cannabis and people who do not use cannabis.
| Agree(%) | |||
|---|---|---|---|
| Attitude statement | All respondents | People who use cannabis | People who do not use cannabis |
|
Using cannabis can be beneficial |
77.2% | 95% | 73.8% |
|
It would be easy for me to access cannabis in the next 24 hours |
70% | 91.4% | 65.2% |
|
Using cannabis is socially acceptable |
65% | 85.1% | 62.2% |
|
I see advertisements for cannabis regularly |
26.4% | 22.5% | 28% |
|
Cannabis use is a problem in my community |
22.9% | 8.7% | 25.1% |
|
I would give someone under 19 cannabis if I had some to share |
7.6% | 15% | 2.7% |
Note: Table includes people who ‘strongly agree’ and ‘somewhat agree’
Note: All differences between people who use cannabis and people who do not are statistically significant.
Most participants believed that cannabis use can be beneficial, that it would be easy for them to access cannabis, and that using cannabis is socially acceptable. These results highlight opportunities for WDGPH and partners to promote healthier attitudes toward recreational cannabis use. In contrast, few respondents agreed that they see advertisements for cannabis regularly (26.4%), or that cannabis use is a problem in their community (22.9%).
Attitudes differed between people who had used cannabis in the past year, and people who had not. Cannabis users were more likely to agree with positive statements about cannabis (e.g. “Using cannabis can be beneficial”) and less likely to agree with negative statements (e.g. “Cannabis use is a problem in my community”). Additionally, 15% of cannabis users indicated a willingness to share cannabis with an underage person, in contrast to less than 3% of cannabis non-users.
Lifetime Cannabis Use
Three quarters of respondents (74.2%) reported that they had used non-medical cannabis in their lifetime. About one-half of these people had begun to use cannabis prior to or at age 16. Fewer than one in ten began using cannabis after age 25 – the age at which the teenage brain stops developing.8
Figure 1. Age of first use of cannabis among respondents who have ever used cannabis (weighted)
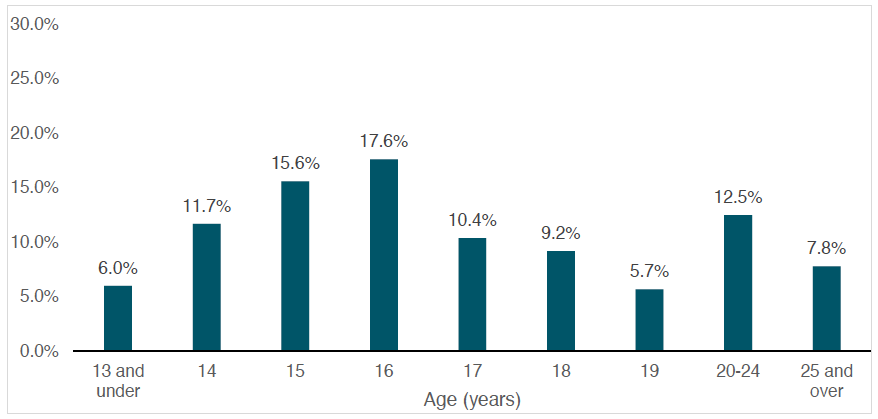
| Age (Years) | Percent (%) |
|---|---|
| 13 and under | 6.0% |
| 14 | 11.7% |
| 15 | 15.6% |
| 16 | 17.6% |
| 17 | 10.4% |
| 18 | 9.2% |
| 19 | 5.7% |
| 20-24 | 12.5% |
| 25 and over | 7.8% |
Past-Year Cannabis Use
Over one-third of respondents (38.3%) reported using cannabis in the past year. This proportion is much higher than recent Canadian-wide surveys that suggest approximately 15 to 22 percent of the population has used cannabis in the past 12 months. 5,6,7 Many of these respondents reported using cannabis either less than one day per month (26.9%) or using cannabis daily (25.2%). (Figure 2).
Figure 2. Frequency of cannabis use among respondents who used cannabis in the past 12 months (weighted)
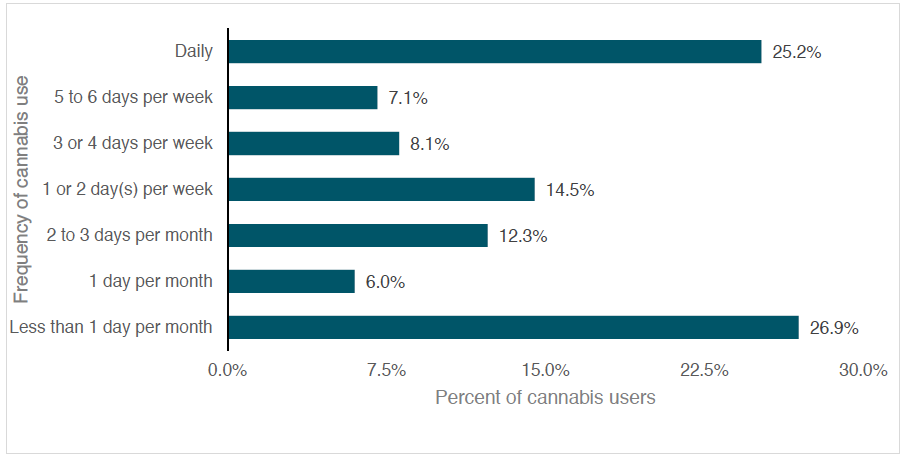
| Frequency of cannabis use | Percent of cannbis uers |
|---|---|
| Less than 1 day per month | 26.9% |
| 1 day per month | 6.0% |
| 2 to 3 days per month | 12.3% |
| 1 or 2 day(s) per month | 14.5% |
| 3 or 4 days per week | 8.1% |
| 5 to 6 days per week | 7.1% |
| Daily | 25.2% |
Figure 3 shows the frequency of cannabis use among respondents who used cannabis in the past year, by age group. Daily cannabis use was highest among respondents aged 30 to 39 (34.2%).
Figure 3. Daily cannabis use among people who used cannabis in the last 12 months, by age group (weighted)
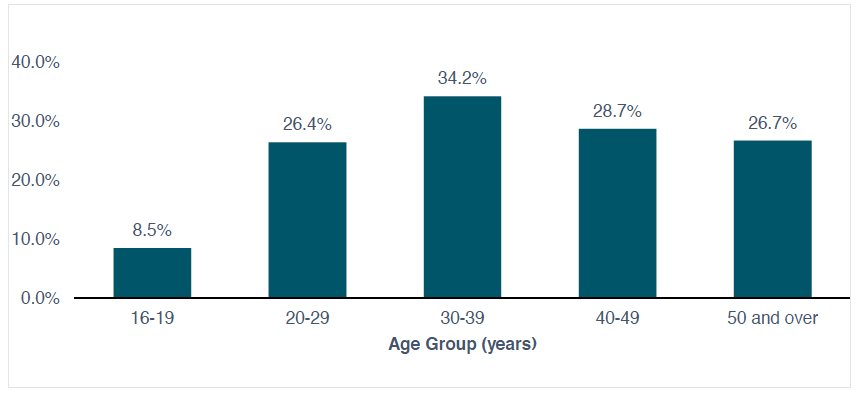
| Age Group (years) | Percent (%) |
|---|---|
| 16-19 | 8.5% |
| 20-29 | 26.4% |
| 30-39 | 34.2% |
| 40-49 | 28.7% |
| 50 and over | 26.7% |
Note: Total for each age group may not add up to 100 percent due to rounding.
Cannabis use and driving
Among respondents who reported using cannabis in the past year, almost one-quarter (24.3%) reported that they have driven a motor vehicle within two (2) hours of using cannabis.
Intention to use among people who do not use cannabis
Over half of respondents that had not used cannabis in the past year (55.4%) reported that they are unlikely to use cannabis once it is legal in Ontario. These respondents were less likely to express an interest in trying edible cannabis products once legal, compared to respondents who already used cannabis.
Preferred communication methods for cannabis information
Respondents were asked to indicate their preferred ways to receive useful and accurate information to them about cannabis. Table 3 shows the top communication methods reported by respondents. The preferred way to receive cannabis information may not correlate with the most accurate as the cannabis industry has a direct conflict in providing this information. This may indicate that the cannabis industry is providing the preferred source of information about cannabis which is a concerning trend.
| Communication method | Percent |
|---|---|
|
In stores that sell cannabis, if legalized |
55.2% |
|
WDG Public Health’s social media (e.g. Facebook, Twitter) |
40.6% |
|
Television advertising |
39.5% |
|
Doctors’ appointment |
38.9% |
|
YouTube |
36.3% |
|
Radio advertising or announcements |
34.4% |
Note: Total percent does not add up to 100% as respondents were able to select more than one response.
Conclusion
The WDG Cannabis Survey recruited 2,776 valid and complete responses, which were weighted to be more representative of the WDG population. Over one-third of respondents reported they had used non-medical cannabis in the past year. Based on other Canadian cannabis surveys this number is expected to be between 15 and 22 percent, suggesting this survey attracted a high number of people who use cannabis.
Knowledge about some aspects of cannabis use was poor, and knowledge was lower among cannabis users than non-users. Fewer than two-thirds of all respondents knew that:
- Using cannabis while pregnant can cause harm to the fetus/child,
- Using cannabis daily or almost daily can cause problems with memory, learning and decision-making,
- Using high doses of cannabis can cause psychosis,
- Using cannabis can result in dependence or addiction, and
- Cannabis smoke has many of the same cancer-causing chemicals as tobacco smoke.
These knowledge gaps are an opportunity to offer targeted and accurate information to the public to promote safer cannabis use. Survey results informed the focus and key messages of the recent ‘Talking About Weed’ awareness campaign. WDGPH will continue to use the survey results to shape programs and services to reduce cannabis-related harms.
Baseline data collected in this survey can be compared to data collected in future (post-legalization) surveys to assess the impacts of cannabis legalization. WDGPH will also share survey results with municipalities and health and social service providers to help inform community policies and programs relating to cannabis use.
Ontario Public Health Standards
Foundational Standards:
Population Health Assessment
Goal: Public health practice responds effectively to current and evolving conditions and contributes to the public’s health and well-being with programs and services that are informed by the population’s health status, including social determinants of health.
Health Equity
Goal: Public health practice results in decreased health inequities such that everyone has equal opportunities for optimal health and can attain their full health potential without disadvantage due to social position or other socially determined circumstances.
Effective Public Health Practice
Goal: Public Health practice is transparent, responsive to current and emerging evidence, and emphasizes continuous quality improvement.
Program Standards
Substance Use and Injury Prevention
Goal: To reduce the burden of preventable injuries and substance use.
Requirements:
- The board of health shall collect and analyze relevant data to monitor trends over time, emerging trends, priorities, and health inequities related to injuries and substance use and report and disseminate the data and information in accordance with the Population Health Assessment and Surveillance Protocol, 2018 (or as current).
- The board of health shall develop and implement a program of public health interventions using a comprehensive health promotion approach that addresses risk and protective factors to reduce the burden of preventable injuries and substance use in the health unit population.
WDGPH Strategic Direction(s)
Health Equity: We will provide programs and services that integrate health equity principles to reduce or eliminate health differences between population groups.
Organizational Capacity: We will improve our capacity to effectively deliver public health programs and services.
Service Centred Approach: We are committed to providing excellent service to anyone interacting with WDG Public Health.
✓ Building Healthy Communities: We will work with communities to support the health and well-being of everyone.
Health Equity
There are several populations that are more vulnerable to cannabis-related harms. People aged 15 to 24 years of age are more likely to use cannabis and they are more likely to experience cannabis-related harms as their brains are still developing.9 Youth who begin using cannabis regularly at a young age are at an increased risk for developing an addiction, mental health issues and learning and memory problems.8,9 This could be of concern in WDG as the survey results show that age of first use of cannabis peaks at 16 years of age, and youth are using cannabis more frequently on a weekly basis (i.e. 1 to 6 days per week) compared to older age groups.
Additionally, using cannabis while pregnant can lead to lower birth weight and has been associated with long-term developmental impacts in children and adolescents (e.g. decrease in memory, ability to pay attention and reasoning and problem-solving skills).8 Lastly, people who have a personal or family history of mental health issues (especially psychosis or substance use disorder) have an increased risk of developing mental illnesses, like psychosis or schizophrenia.8
Portions of the recent ‘Talking About Weed’ awareness campaign address high-risk groups, including youth, people who are pregnant and people with personal or family history of mental illness. Moving forward, communicating survey results internally, with community partners and the public will allow for more targeted health promotion communication and improvements to programs and services for these high-risk groups. Lastly, continued monitoring of cannabis use patterns among these high-risk groups will assist with understanding how cannabis legalization will impact them.
References
- Government of Canada, Department of Justice. Cannabis Legalization and Regulation [Internet]. 2018 Oct 17 [cited 2018 Oct 31]. Available from: https://www.justice.gc.ca/eng/cj-jp/cannabis/
- Government of Ontario. Cannabis Legalization [Internet]. 2018 Oct 29 [cited 2018 Oct 31]. Available from: https://www.ontario.ca/page/cannabis-legalization
- Popova S, Giesbrecht N, Bekmuradov D, Patra J. Hours and days of sale and density of alcohol outlets: Impacts on alcohol consumption and damage: A systematic review. Alcohol and Alcoholism [Internet]. 2009 [cited 2018 Nov 3]; 44 (5): 500-516. Available from: https://academic.oup.com/alcalc/article/44/5/500/182556
- Smoke-Free Ontario Scientific Advisory Committee, Ontario Agency for Health Protection and Promotion. Evidence to Guide Action: Comprehensive Tobacco Control in Ontario (2016) [Internet]. 2017 Apr [cited 2018 Nov 3]. Available from: https://www.publichealthontario.ca/en/eRepository/SFOSAC%202016_FullReport.pdf
- Government of Canada. Canadian Tobacco, Alcohol and Drugs Survey: Summary of results for 2017 [Internet]. 2018 Nov 7 [cited Nov 20]. Available from: https://www.canada.ca/en/health-canada/services/canadian-tobacco-alcohol-drugs-survey/2017-summary.html
- Statistics Canada. National Cannabis Survey, second quarter 2018 [Internet]. 2018 Aug 9 [cited 2018 Oct 19]. Available from: https://www150.statcan.gc.ca/n1/daily-quotidien/180809/dq180809a-eng.htm
- Government of Canada. Canadian Cannabis Survey 2018 Summary [Internet]. 2018 Nov 19 [cited 2018 Oct 19]. Available from: https://www.canada.ca/en/services/health/publications/drugs-health-products/canadian-cannabis-survey-2018-summary.html
- Government of Canada. Health Effects of Cannabis [Internet]. [cited 2018 Nov 5]. Available from: https://www.canada.ca/content/dam/hc-sc/documents/services/campaigns/27-16-1808-Factsheet-Health-Effects-eng-web.pdf
- Canadian Centre on Substance Abuse. Substance abuse in Canada: The effects of cannabis use during adolescence [Internet]. 2015 [cited 2018 Nov 5]. Available from: http://www.ccsa.ca/Resource%20Library/CCSA-Effects-of-Cannabis-Use-during-Adolescence-Report-2015-en.pdf
Appendices
Appendix “A” – Cannabis Survey Results
Appendix “A”
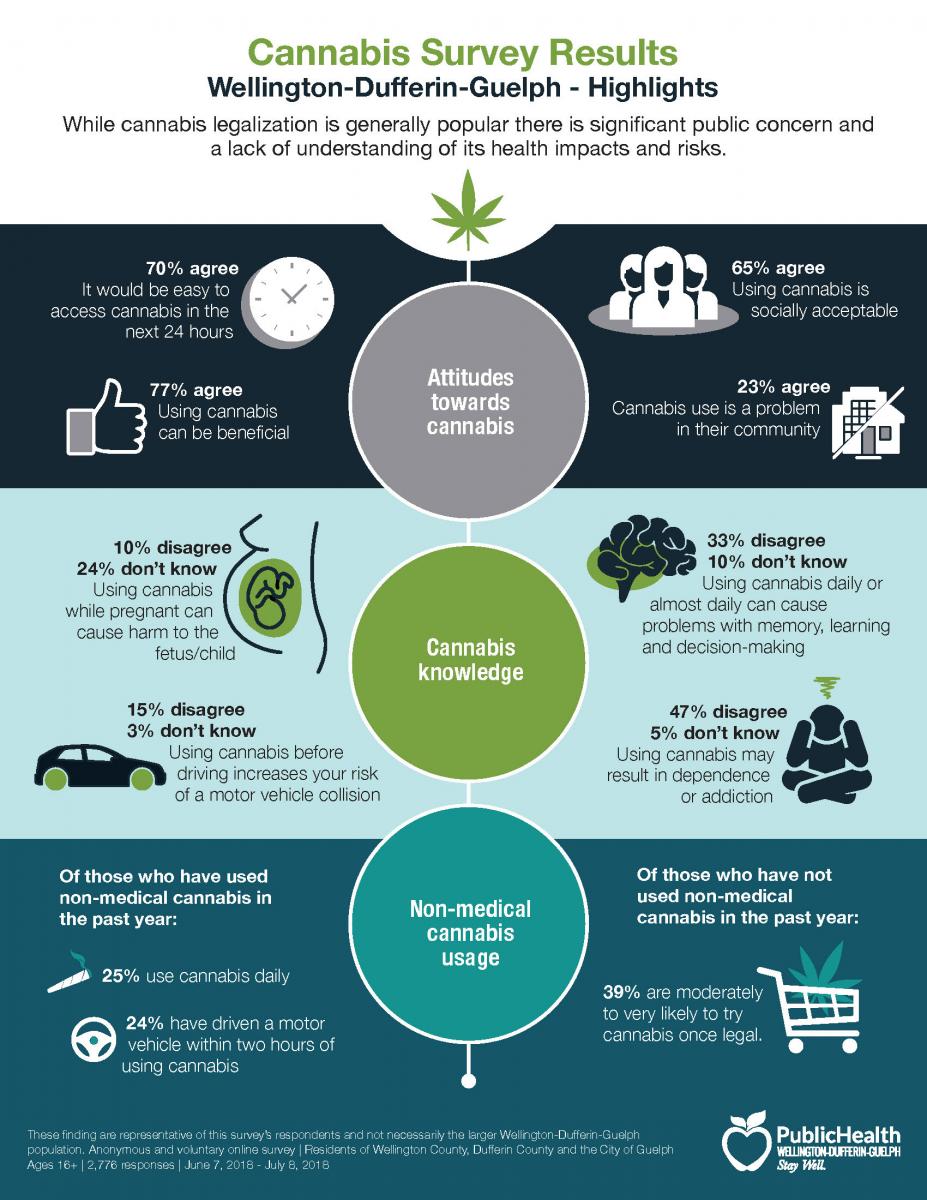
Cannabis Survey Results
Wellington-Dufferin-Guelph Highlights
While cannabis legalization is generally popular there is significant public concern and a lack of understanding of its health impacts and risks.
Attitudes towards cannabis
- 70% agree it would be easy to access cannabis in the next 24 hours
- 77% agree using cannabis can be beneficial
- 65% agree using cannabis is socially acceptable
- 23% agree cannabis use is a problem in their community
Cannabis knowledge
- 10% disagree and 24% don’t know using cannabis while pregnant can cause harm to the fetus/child
- 15% disagree and 3% don’t know using cannabis before driving increases your risk of a motor vehicle collision
- 33% disagree and 10% don’t know using cannabis daily or almost daily can cause problems with memory, learning and decision-making
- 46% disagree and 5% don’t know using cannabis may result in dependence or addiction
Non-medical cannable usage
Of those who have used non-medical cannabis in the past year:
- 25% use cannabis daily
- 24% have driven a motor vehicle within two hours of using cannabis
Of those who have not used non-medical cannabis in the past year:
- 36% are moderately to very likely to try cannabis once legal.