Meeting date: September 5, 2018
Report No.: BH.01.SEP0518.R20
Prepared by: Liz Robson, Manager, Family Health Promotion
Approved by: Andrea Roberts, Director, Family Health
Submitted by: Dr. Nicola J. Mercer, MD, MBA, MPH, FRCPC, Medical Officer of Health and CEO
Recommendations
It is recommended that the Board of Health:
- Receive this report for information.
Key Points
- From 2016-2017, Wellington-Dufferin-Guelph Public Health (WDGPH) completed a process and outcome evaluation of the in-person prenatal program.
- Ten recommendations emerged from the evaluation. To date, six of the recommendations have been fully implemented, two are in progress and the remaining two will be completed by the end of 2018.
- Program changes implemented January 1, 2018 have already demonstrated improved value for money. The revised program and schedule has reduced instructional hours for the program by up to 74% without negatively impacting registration numbers and participant learning.
- Program changes implemented January 1, 2018 have resulted in zero class cancellations to date in 2018. This has eliminated the administrative burden associated with class cancellations.
- It is recognized that the in-person prenatal program does not meet the needs of all priority populations in the Wellington-Dufferin-Guelph (WDG) community including youth under the age 24, low-income households, single individuals, individuals with less than high school education and unemployed individuals. WDGPH is developing new strategies to better reach these individuals prior to and during pregnancy as they are at greater risk of adverse prenatal and childbirth outcomes.
Discussion
About the In-Person Prenatal Program
The Ontario Public Health Standards (2018), provides requirements for programs, services and accountability for public health units in Ontario. Within the Healthy Growth and Development Standard, there is a requirement for boards of health to develop and implement a program of public health interventions using a comprehensive health promotion approach to support healthy growth and development.1 Boards of health are required to consider the topic areas of healthy pregnancies, breastfeeding, growth and development, mental health promotion, preparation for parenting and positive parenting based on an assessment of local needs. An evaluation of the WDGPH in-person prenatal program was undertaken to better understand the local need for this program in the WDG community.
Studies show that prenatal education increases knowledge, the likelihood of being in active labour when arriving at the hospital, and rates of breastfeeding initiation and continuation.2,3 Prenatal education also improves maternal mental health and mental readiness for childbirth, decreases use of epidurals, and increases satisfaction about couple and parent-infant relationships after birth.3 As a result, prenatal education has the potential to positively impact individuals, families and society. Capitalizing on this opportunity requires WDGPH to determine the specific role that an in-person prenatal program has in the larger context of community programs and services in addition to a population health approach to improving healthy pregnancies.
The in-person prenatal program at WDGPH is facilitated by a registered nurse (RN). Each group session incorporates a variety of information sharing methods, including videos, activities and group discussions. WDGPH continuously monitors registration numbers to assess if the changing landscape for information sharing including websites, social media and apps has an influence on this program.
In-Person Prenatal Program Evaluation
From 2016-2017, WDGPH completed a process and outcome evaluation to answer the following questions about the in-person prenatal program:
- How does the WDGPH prenatal program currently operate?
- What impact is the prenatal program having on participants?
- Is there still a need for the prenatal program in the community?
- How can the prenatal program be improved?
- How do other central west and south west public health unit prenatal programs operate?
To answer these questions, WDGPH developed a comprehensive evaluation plan and collected both quantitative and qualitative data from seven different sources. Evaluation data collection methods are summarized in Table 1.
| Data Source | Number of Participants | Data Collection Method |
|---|---|---|
| Program participants (expectant women) | 100 | In-class evaluation survey administered at the end of the last class |
| Program participants (partners and support people) | 97 | In-class evaluation survey administered at the end of the last class |
| First time mothers | 184 | Telephone survey administered at 2 months postpartum |
| Local healthcare providers | 33 | Surveys administered online or in hard copy |
| Other public health unit prenatal programs | 15 | Telephone interviews with other public health units |
| Local prenatal programs | 3 | Telephone interviews with local private prenatal programs |
| Program facilitators, program manager and prenatal lead | 5 | In-person interviews |
An evaluation report was prepared that describes in detail the findings from the evaluation.4 Overall, the evaluation concluded that there is still a need for the program in the community. Ten recommendations were developed to improve the program. A summary of these recommendations and actions taken are summarized in Table 2.
| Recommendation | Status | Actions Taken |
|---|---|---|
| Update class content and delivery of information to meet client needs, and to build hands-on and informed decision making skills | Complete |
Curriculum completely revised. Instructional time for program reduced from 12 hours to 6 hours. New program emphasizes a hybrid approach to learning by pairing an online program with the in-person education. New program launched January 1, 2018. |
| Increase transparency of payment options and ease of registrations for clients experiencing financial hardship | Complete | As a result of partnerships with EarlyON, the in-person prenatal program is available at no cost to all program participants as of June 28, 2018. |
| Consider additional or alternate locations for the in-person prenatal program in Guelph and Fergus so as to meet clients’ expressed needs and preferences | Complete |
Guelph program moved to EarlyON at Stone Road Mall as of June 2018. No need to relocate Fergus program at this time. |
| Explore alternate staffing arrangements to improve challenges with retention, scheduling and content expertise | Complete | Program is now delivered by a mix of public health nurses and casual prenatal facilitators |
| Implement strategies that will increase local healthcare provider awareness, support, promotion and client referral to prenatal education. | Complete | New prenatal referral form developed and promoted with healthcare providers including physicians, obstetricians, midwives, nurse practitioners and nurses throughout WDG. |
| Design and implement an ongoing program evaluation plan for continuous monitoring of class process, outcome indicators and quality improvement. | Complete |
First formative evaluation for the newly launched curriculum took place from January – June 2018. WDGPH is committed to an ongoing and iterative cycle for program evaluation. |
| Develop a new model for prenatal education delivery outside of Guelph, Orangeville and Fergus. | In progress | Will be developed by the end of 2018. |
| Develop a new model to deliver prenatal education to priority populations including youth (under 24 years) and low income households. | In progress | Will be developed by the end of 2018. |
| Support community partners (e.g. community centres, libraries, labs, doulas, etc.) to promote the prenatal program with their clients. | In progress | Scheduled to begin Q4 2018. |
| Assess local interest in the establishment of a prenatal service provider’s network. | In progress | Scheduled to begin Q4 2018. |
Impact of Program Changes
As a result of the prenatal evaluation, WDGPH has been able to implement significant changes to the in-person prenatal program. One of the changes that took effect January 1, 2018, has been the movement to a hybrid model that emphasizes participation in both an online and in-person program. This change has allowed the in-person program to be reduced from 12 hours of instructional time to 6 hours. The Saturday class offering was also discontinued as of January 1, 2018 with classes now only running on weekday evenings. These changes to both the instructional time and the schedule have reduced instructional hours for the program by up to 74% from a high of 672 hours in 2015 to 174 hours in 2018.
The value in these changes are that even with a significant reduction in instructional time and class offerings, it is projected that WDGPH will reach slightly more individuals through the in-person program in 2018 compared to previous years (see Figure 1). In addition, these changes have resulted in a streamlined schedule that has seen zero cancellations to date in 2018, where previous years have seen up to 21 series cancelled (see Table 3). Cancellations previously had a large administrative burden which involved contacting participants, issuing refunds and re-scheduling clients. With zero class cancellations projected in 2018, this will result in time savings for the Family Health program assistant.
In addition to financial savings achieved through the in-person prenatal evaluation, the formative evaluation has demonstrated that program participants continue to learn new information through the program. For example, 93 to 95% of participants agreed that they learned new strategies to help them prepare for labour and birth, breastfeeding and early parenting through the revised curriculum.
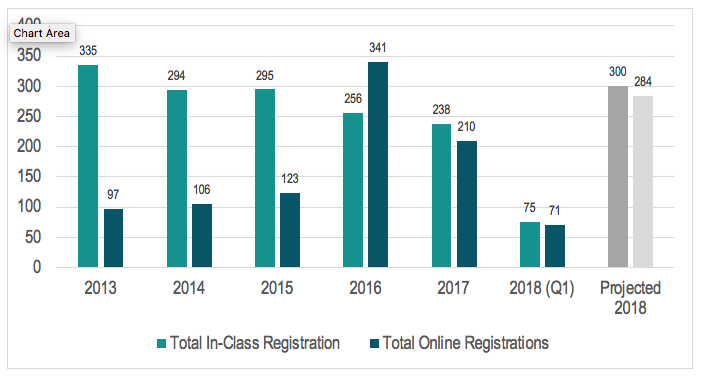
2013 - In-Class: 335, Online: 97
2014 - In-Class: 294, Online: 106
2015 - In-Class: 295, Online: 123
2016 - In-Class: 256, Online: 341
2017 - In-Class: 238, Online: 210
2018 (Q1) - In-Class: 75, Online: 71
Projected 2018: In-Class: 300, Online: 284
| Year | Number of Series Scheduled | Number of Series Cancelled |
|---|---|---|
| 2015 | 56 | 21 |
| 2016 | 49 | 21 |
| 2017 | 39 | 11 |
| 2018 (Q1 only) | 8 | 0 |
| 2018 (Projected) | 29 | 0 |
Conclusion
The in-person prenatal evaluation demonstrates the importance of evaluation as part of an ongoing and iterative cycle of program development and improvement.1 WDGPH continues to be adaptive to the changing needs of the community from an individual to a systematic level when planning and implementing interventions with the aim of contributing to healthy pregnancies. The in-person prenatal evaluation led to significant program changes that have improved the value for money of the program without negatively impacting registration numbers and client preparedness for labour and birth, breastfeeding and early parenting. WDGPH is currently planning new strategies to better meet the needs of pregnant priority populations throughout WDG.
Ontario Public Health Standard
Foundational Standard:
Health Equity
Goal: Public health practice results in decreased health inequities such that everyone has equal opportunities for optimal health and can attain their full health potential without disadvantage due to social position or other socially determined circumstances.
Effective Public Health Practice
Goal: Public health practice is transparent, responsive to current and emerging evidence, and emphasizes continuous quality improvement.
Program Standards:
Healthy Growth and Development
Goal: To achieve optimal preconception, pregnancy, newborn, child, youth, parental, and family health.
WDGPH Strategic Direction(s)
✓ Health Equity: We will provide programs and services that integrate health equity principles to reduce or eliminate health differences between population groups.
✓ Organizational Capacity: We will improve our capacity to effectively deliver public health programs and services.
✓ Service Centred Approach: We are committed to providing excellent service to anyone interacting with WDG Public Health.
✓ Building Healthy Communities: We will work with communities to support the health and well-being of everyone.
Health Equity
The in-person prenatal evaluation identified that most participants of the in-person prenatal program are aged 30 years or older (88%), have a household income of greater than $80,000 per year (65%) and are expecting their first baby (95%).4 Research confirms that these results are consistent with trends from the rest of the province, as the following groups are more likely than their counterparts to participate in a prenatal class in Ontario: people aged 25-34, individuals expecting their first baby, and people living in higher income neighbourhoods.5
This data also provides insight into those not attending the WDGPH in-person prenatal program. Currently the program is not reaching many young parents. Only 7% of survey participants were between the ages of 20 and 24 years and none were less than 20 years. The program is also not reaching many people of low income (making less than $39,999 a year in household income). Research confirms that several groups of women are found to be less likely to receive prenatal education including low income, single, less than high school education and unemployed.5 As these women are at greater risk of adverse prenatal and childbirth outcomes, more must be done to connect and provide information prior to and during pregnancy.5
To reduce these health inequities, WDGPH is currently developing a new model to deliver prenatal education to priority populations including youth (under 24 years) and low income households. This model will be developed by the end of Q4 2018 (See Table 2).
References
- Ontario. Ministry of Health and Long-Term Care. Ontario Public Health Standards: Requirements for Programs, Services and Accountability. 2018. Toronto, ON: Queen’s Printer for Ontario; 2018 [cited 2018 July 13]. Available from: http://www.health.gov.on.ca/en/pro/programs/publichealth/oph_standards/docs/protocols_guidelines/Ontario_Public_Health_Standards_2018_en.pdf
- Godin, K; Blue, S; Bourdages, N; Edwards, S; Horan, M; MacDougall, R; Mill, C; Procter, TD; Schieck, A; Alton, GD. Assessing Public Health Prenatal Education Knowledge: Findings from the LDCP Healthy Pregnancies Project [Internet]. 2014. [cited 2018 July 13]. Available from: https://www.publichealthontario.ca/en/ServicesAndTools/Documents/LDCP/LDCP_Healthy_Pregnancies_Knowledge_Survey_Report_2014.pdf
- BORN Information System [2013-2015], BORN Ontario [extracted: {7 June 2016}]
- Wellington-Dufferin-Guelph Public Health. 2018. In-Person Prenatal Evaluation Findings. Guelph, Ontario.
- Best Start Resource Centre. Prenatal Education in Ontario: Fact Sheet 1: The Evidence for Prenatal Education [Internet].2014. [cited 2018 July 12]. Available from: https://www.beststart.org/resources/rep_health/BSRC_Prenatal_Fact_Sheet_1_2015.pdf
Appendices
None